
UPDATED PRACTICE GUIDELINES
In response to the COVID-19 pandemic, the out-of-hospital Midwives are modifying our practices to protect our clients and ourselves from COVID-19 infection and transmission. Below are the measures taken to keep everyone safe and healthy during these times.
For example, one of our local hospitals is only having 4 total in-person visits in the entire pregnancy for low risk pregnancies. The first in-person appointment is at 12 weeks (in combination with an NT ultrasound and bloodwork), 18 weeks (in combination with an anatomy ultrasound), 28 weeks (in combination with gestational diabetes testing and 36 weeks (in combination with a GBS test). All other appointments are telemedicine/virtual. We will be offering a slight modification of this reduced schedule based on your needs and previous appointments. These policies may change at a moment’s notice and we continue to be in contact with local local hospitals and public health departments in an attempt to keep everyone as safe as possible. You can ask your midwife at any time about their measures to reduce exposure.
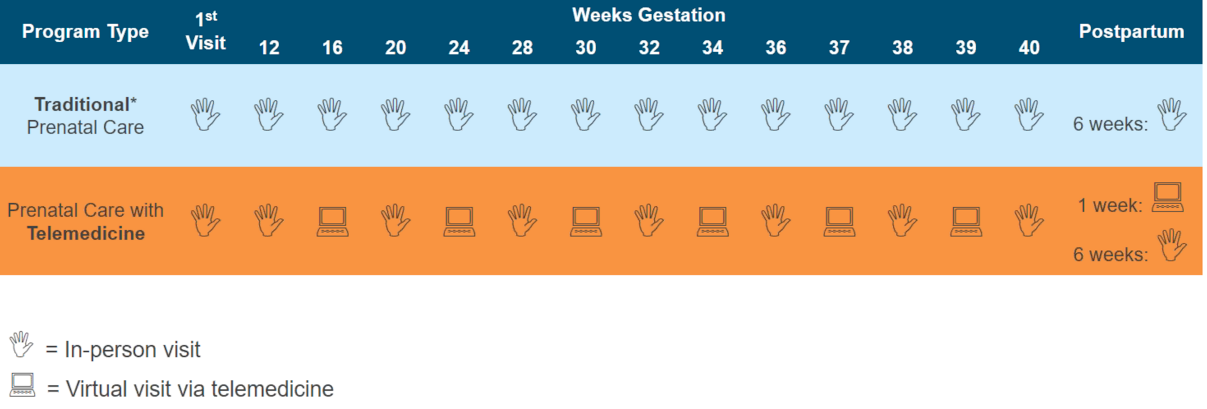
Sample prenatal schedule with Telemedicine (subject to change due to above mentioned variables)
You will be asked to purchase a digital blood pressure cuff, thermometer (that works for babies and adults) and preferably a baby scale to facilitate telemedicine postpartum appointments (a food scale can often substitute). You will be asked to sanitize all hard surfaces in your home before a home appointment and before your midwife(s) arrives in labor.
I cannot see clients for in-person appointments or for labor who:
In order to protect everyone:
If I become ill or are exposed to COVID-19:
What about complications and emergencies?
Some people develop difficulties during their pregnancy or labor, which could increase the risks associated with giving birth at home. If you find yourself facing a potentially problematic situation, I will help you to understand the problem and explore your options. I am able to assist a woman in childbirth so long as progress meets “criteria accepted as normal”. What is “normal” is not legally defined but in the current pandemic it is prudent to be conservative. If a complication arises during my attendance at your labor, I will keep you informed, advise you of risks and assist you in decision-making. Rarely, an emergency will arise suddenly and unexpectedly and must be dealt with immediately. Although homebirth midwives are trained to provide emergency care for the woman and her baby, we cannot duplicate a hospital setting.
We all need to understand that in the event of a surge of sick people in our local area, EMS services (ambulance) may be overwhelmed and potentially even unavailable entirely. We have to be prepared to transport to the hospital in private car and depending on the situation this might not be ideal and has the potential to negatively affect outcomes but might be the best we can do. Also, in order to protect our clients and ourselves, the attending midwife will not transfer into the hospital with you. If by private car, the midwife will assist you to the ER. If by ambulance, the midwife will not assist you. Some hospitals are currently not letting any support persons in with the mother and some are letting one person. These policies are changing rapidly and we can not guarantee who will be allowed into the hospital at your time of birth.
What if I can’t be at your birth?
Fortunately, I have agreements with several midwives to support me in a variety of ways. Together we have a goal of maintaining a network of midwives to support each other as we meet the highest standard of care for our clients. Several midwives regularly assist me at births. I depend on these midwives to support me, as well as you and your family. If it becomes impossible for me to attend your birth, I will call one of these qualified people to take my place. I promise you I will do everything in my power to fulfill my obligation to you. Sometimes two people will be in labor at the same time. They do not often birth at the same time, but this situation can create tension for the families involved. This circumstance is rare. Should this situation arise when you are in labor, I will decide who needs my personal attention most urgently and call another midwife to attend the other family. This decision will be based partly on timing and partly on a woman’s childbearing history and risk factors.
It is possible that during a pandemic several of the local midwives could be sick and there may not be enough midwives for all the births. We will do our best to cover each other’s practices in this situation but if no homebirth midwives are available a hospital birth may be required.
Once in a while, a woman will have a precipitous labor, which is a very short labor where there is no time for a birth attendant to arrive before the baby. I help all families educate and prepare for this possibility just in case it should happen.
The Client will:
By consenting to Care with South Shore Home Birth Midwifery you are agreeing to these terms and conditions which will continue to change per the CDC, ACOG and WHO recommendations. Please check this page regularly for updates.
In response to the COVID-19 pandemic, the out-of-hospital Midwives are modifying our practices to protect our clients and ourselves from COVID-19 infection and transmission. Below are the measures taken to keep everyone safe and healthy during these times.
- We are reducing the number of in-person appointments both in pregnancy and postpartum per ACOGs recommendations. This is a strategy to reduce everyone’s exposures. Every person to person contact is a risk factor for infection during a pandemic. The other regularly scheduled appointments will be virtual.
For example, one of our local hospitals is only having 4 total in-person visits in the entire pregnancy for low risk pregnancies. The first in-person appointment is at 12 weeks (in combination with an NT ultrasound and bloodwork), 18 weeks (in combination with an anatomy ultrasound), 28 weeks (in combination with gestational diabetes testing and 36 weeks (in combination with a GBS test). All other appointments are telemedicine/virtual. We will be offering a slight modification of this reduced schedule based on your needs and previous appointments. These policies may change at a moment’s notice and we continue to be in contact with local local hospitals and public health departments in an attempt to keep everyone as safe as possible. You can ask your midwife at any time about their measures to reduce exposure.
Sample prenatal schedule with Telemedicine (subject to change due to above mentioned variables)
You will be asked to purchase a digital blood pressure cuff, thermometer (that works for babies and adults) and preferably a baby scale to facilitate telemedicine postpartum appointments (a food scale can often substitute). You will be asked to sanitize all hard surfaces in your home before a home appointment and before your midwife(s) arrives in labor.
I cannot see clients for in-person appointments or for labor who:
- Have cough, runny nose, fever, vomiting or diarrhea
- Have had exposure to people with these symptoms in the previous 14 days
- Have had exposure to a person with a known COVID-19 infection in the past 14 days
- If any of the above are true at the time of labor, a hospital birth will be required
In order to protect everyone:
- Temperatures of everyone present at in-person appointments will need to be taken and at labors (including myself and fellow midwives) and if an elevated temperature is present in anyone, your appointment will be rescheduled and if you are in labor, your care will be transferred to a hospital provider.
- We ask that you do not bring your kids or partners to any appointments.
- For clinic visits we ask that you wash your hands immediately upon arrival.
- We will maintain 6' distance from each other until the physical exam which will take place with gloves and mask.
- We will disinfect all equipment used between each person and wipe down all hard surfaces and doorhandles.
- For in-home visits our clothes will be changed in between visits.
- Labor in water is safe. But there is possible transmission of Covid-19 through fecal matter. SSHB birth tubs are used by families in the SSHB practice, even with a new liner, using one of SSHB birthing pools needs to be a personal decision. The pools are sanitized to the best of my ability after each use, but cannot be guaranteed to be safe from all contaminants.
- Only essential people are allowed at the birth. We ask that you consider the health of your midwives and all the other families and newborns in our care when deciding on who you invite to your birth.
- No visitors in the postpartum until the shelter-in-place is lifted.
If I become ill or are exposed to COVID-19:
- If I (or any of my family members) have any symptoms as described above, I will cancel all appointments until medically cleared to begin seeing clients
- If I (or anyone of my family members) have known exposure to anyone with symptoms, I will cancel all appointments until 14 days after exposure
- If we must cancel, we will make every effort to find you another caregiver or arrange to see you virtually (if virtual care is appropriate for your situation)
- I am limiting my only contacts to necessary client appointments and births and otherwise am self-quarantining.
What about complications and emergencies?
Some people develop difficulties during their pregnancy or labor, which could increase the risks associated with giving birth at home. If you find yourself facing a potentially problematic situation, I will help you to understand the problem and explore your options. I am able to assist a woman in childbirth so long as progress meets “criteria accepted as normal”. What is “normal” is not legally defined but in the current pandemic it is prudent to be conservative. If a complication arises during my attendance at your labor, I will keep you informed, advise you of risks and assist you in decision-making. Rarely, an emergency will arise suddenly and unexpectedly and must be dealt with immediately. Although homebirth midwives are trained to provide emergency care for the woman and her baby, we cannot duplicate a hospital setting.
We all need to understand that in the event of a surge of sick people in our local area, EMS services (ambulance) may be overwhelmed and potentially even unavailable entirely. We have to be prepared to transport to the hospital in private car and depending on the situation this might not be ideal and has the potential to negatively affect outcomes but might be the best we can do. Also, in order to protect our clients and ourselves, the attending midwife will not transfer into the hospital with you. If by private car, the midwife will assist you to the ER. If by ambulance, the midwife will not assist you. Some hospitals are currently not letting any support persons in with the mother and some are letting one person. These policies are changing rapidly and we can not guarantee who will be allowed into the hospital at your time of birth.
What if I can’t be at your birth?
Fortunately, I have agreements with several midwives to support me in a variety of ways. Together we have a goal of maintaining a network of midwives to support each other as we meet the highest standard of care for our clients. Several midwives regularly assist me at births. I depend on these midwives to support me, as well as you and your family. If it becomes impossible for me to attend your birth, I will call one of these qualified people to take my place. I promise you I will do everything in my power to fulfill my obligation to you. Sometimes two people will be in labor at the same time. They do not often birth at the same time, but this situation can create tension for the families involved. This circumstance is rare. Should this situation arise when you are in labor, I will decide who needs my personal attention most urgently and call another midwife to attend the other family. This decision will be based partly on timing and partly on a woman’s childbearing history and risk factors.
It is possible that during a pandemic several of the local midwives could be sick and there may not be enough midwives for all the births. We will do our best to cover each other’s practices in this situation but if no homebirth midwives are available a hospital birth may be required.
Once in a while, a woman will have a precipitous labor, which is a very short labor where there is no time for a birth attendant to arrive before the baby. I help all families educate and prepare for this possibility just in case it should happen.
The Client will:
- Embrace your responsibility as your own best care provider and respect your inner knowledge and intuition.
- Actively promote a healthy pregnancy by nourishing and exercising your body and mind in ways that are appropriate.
- Identify a support person/s whose main concern is the support of the client throughout pregnancy, labor, birth, and the early postpartum period.
- Provide complete records from other health care providers by our initial visit.
- Become educated about pregnancy, childbirth and infant care through classes, readings and discussions.
- Communicate openly and provide honest and accurate information in all aspects of your health and wellness.
- Have required telemedicine supplies available by our first appointment, unless other arrangements have been made.
- Have required home birth supplies ready by 36 weeks or labor. If you do not have the required supplies, I will not be able to attend you at home.
- Arrange for an adult other than the primary support person to be responsible for any small children who will be present at the labor and birth.
- Adhere to our financial agreement.
By consenting to Care with South Shore Home Birth Midwifery you are agreeing to these terms and conditions which will continue to change per the CDC, ACOG and WHO recommendations. Please check this page regularly for updates.